Curative but Unaffordable: Gene and Cell Therapy's Access Paradox in Asia
03 June 2026 | Wednesday | Analysis

At almost every cell-and-gene-therapy conference in the region, the same slide appears: a child who was dying of leukaemia, now in durable remission; a teenager freed from a lifetime of blood transfusions; a graph where the survival curve simply stops falling. The room applauds. Then the lights come up, and a different number flashes on a payer's spreadsheet down the hall — a price tag with six or seven figures — and the applause turns into arithmetic that almost never works.
This is the access paradox at the heart of cell and gene therapy (CGT) in Asia. The therapies are, in the most literal sense, miraculous: single administrations that can correct the root cause of a disease the patient would otherwise carry for life. But they have arrived inside health systems that were designed, financed, and staffed for the opposite problem — chronic conditions managed with cheap, repeatable treatment. A cure that costs as much as a small apartment block does not fit that machinery. And in much of Asia, where a year of public health spending per person can be measured in tens of dollars, it does not fit by several orders of magnitude.
What follows is an attempt to hold both truths at once: that these therapies are among the most important medical advances of the century, and that, as currently priced and delivered, they will reach only a vanishingly small share of the patients who clinically qualify. The interesting part is what happens next — because Asia is becoming the most important laboratory in the world for the question of whether a curative therapy can also be an affordable one.
The promise: cures aimed squarely at Asia's disease burden
The clinical case for CGT is not theoretical, and crucially, some of its strongest applications map directly onto diseases that are disproportionately Asian.
Start with the haemoglobinopathies. Beta-thalassaemia and sickle cell disease are inherited disorders of haemoglobin, and the thalassaemias in particular are concentrated across the Indian subcontinent, Southeast Asia, the Middle East and the Mediterranean. India alone is estimated to carry roughly a quarter of the global thalassaemia burden, with something like 100,000 to 150,000 people living with the disease and 10,000 to 15,000 children born with it every year; the country has tens of millions of carriers. For these patients, "treatment" has historically meant transfusions every few weeks for life, iron-chelation drugs to manage the resulting overload, and — for the lucky minority with a matched donor and the money — a bone-marrow transplant.
Into that picture arrives Casgevy (exagamglogene autotemcel), the first CRISPR-based medicine ever approved, which edits a patient's own stem cells to switch fetal haemoglobin back on. In its pivotal trials it freed the large majority of transfusion-dependent thalassaemia patients from transfusions and eliminated the severe pain crises of sickle cell disease for most recipients. A disease that demanded lifelong management was, for these patients, simply switched off. Britain's NICE — after initially rejecting it for sickle cell — endorsed Casgevy for transfusion-dependent thalassaemia, an unusually clear signal that a one-shot gene edit can clear a conservative cost-effectiveness bar when the lifetime burden it displaces is large enough.
The second pillar is blood cancer. CAR-T therapy — in which a patient's T cells are re-engineered to hunt CD19-bearing malignant cells — has produced response rates in relapsed or refractory B-cell lymphomas and leukaemias that conventional chemotherapy never approached. India's homegrown NexCAR19 reported around a 70% overall response rate in its pivotal trial; Korea's first domestic CAR-T posted complete-response rates in the high 60s to low 80s in diffuse large B-cell lymphoma. These are patients who had effectively run out of options.
And the frontier keeps widening. India's first in-human gene therapy for haemophilia A, run by the Centre for Stem Cell Research at CMC Vellore, used a lentiviral vector to insert a Factor VIII gene into patients' own stem cells; all five participants reached zero annualised bleeding rates across a cumulative follow-up of nearly seven years, ending their dependence on expensive clotting-factor infusions. The same group is now pursuing CRISPR-based approaches to thalassaemia and sickle cell disease. The science, in short, is delivering durable results against precisely the conditions that weigh most heavily on Asian health systems.
The pricing problem: why a cure breaks the math
Here is where the celebration collides with the spreadsheet.
A conventional drug is priced and paid for in flow: a monthly cost, a recurring claim, a budget line that recurs predictably year after year. Health systems — and especially the social-insurance and tax-funded systems common across Asia — are built around exactly this rhythm. A one-time cure inverts it. The entire lifetime value of the therapy, and its entire cost, lands in a single year, on a single patient, on a single budget.
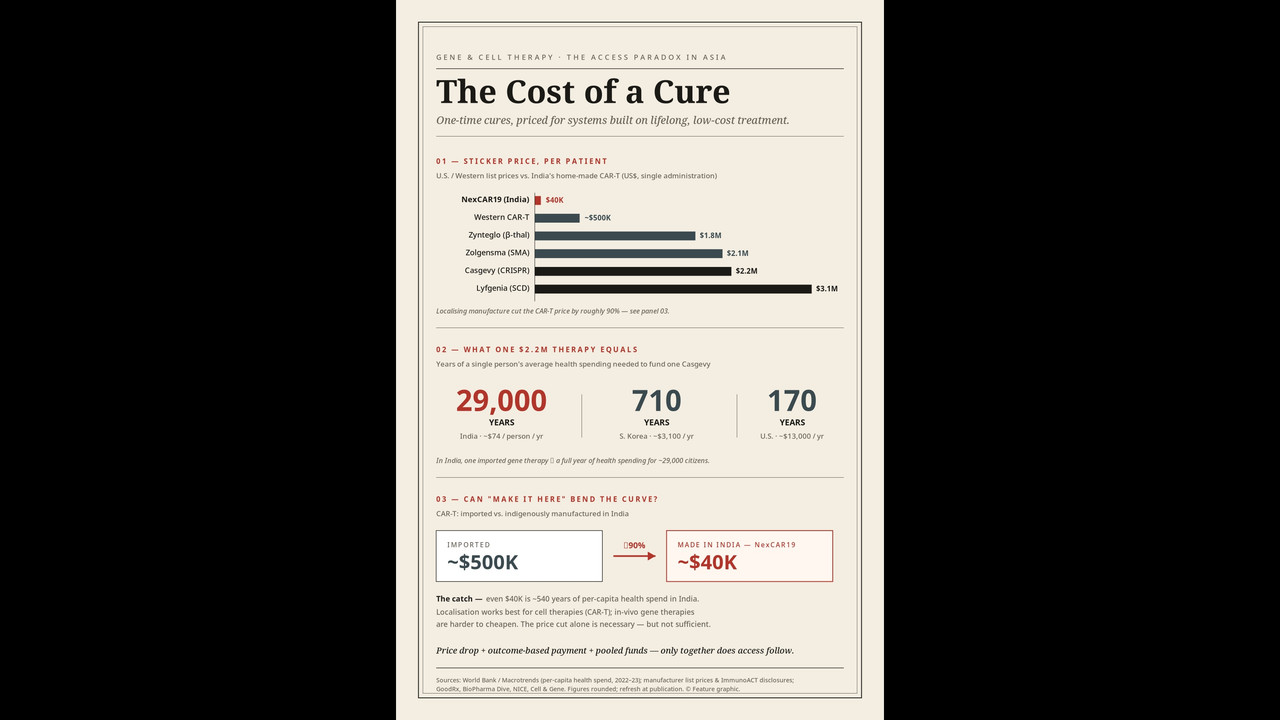
The numbers are staggering on their own terms. Casgevy launched at a U.S. list price of about $2.2 million; its sickle cell competitor, Lyfgenia, at $3.1 million; the spinal muscular atrophy gene therapy Zolgensma at roughly $2.1 million; the thalassaemia gene therapy Zynteglo at $1.8 million. Even "conventional" commercial CAR-T therapies from Western manufacturers run between roughly $370,000 and $530,000 before the considerable hospital and complication costs are added.
Manufacturers defend these figures with a value argument that is not frivolous. The lifetime cost of managing severe sickle cell disease, by Vertex's and Bluebird's own estimates, runs between $4 million and $6 million; against that, a $2–3 million cure can look like a discount, and that is broadly the logic that let it clear a cost-effectiveness threshold in the U.K. But the argument quietly assumes a system that was already spending millions per patient over a lifetime. That assumption simply does not hold across most of Asia.
This is the part that does not translate. Consider the denominators. Annual current health expenditure per person is on the order of $74 in India and around $3,000–3,300 in South Korea, against roughly $13,000 in the United States. A single $2.2 million therapy is therefore equivalent to something like 28,000 years of average per-person health spending in India, or about 700 years in Korea. Put differently: to fund one imported gene therapy at Western list price, India would have to redirect the entire annual health spending of roughly 28,000 of its citizens. No insurance pool, public or private, prices that as a recurring event.
The mismatch is structural, not merely a matter of generosity. Asian financing systems were built to spread small, frequent costs across large populations — the actuarial logic of chronic disease. A curative therapy asks them to absorb an enormous, lumpy, one-time cost for an individual, and to do so before anyone knows whether the "cure" will hold for thirty years or relapse in three. Even where a country can technically afford a handful of cases, the budget-impact uncertainty — how many patients will present, all at once, demanding a multi-million-dollar intervention — is itself disqualifying. The therapy that is too good to be a drug is also, for these systems, too expensive to be a benefit.
The result is a reimbursement vacuum. Across most of Asia, these therapies are approved but not reimbursed, or available only through private payment and patient-assistance schemes. China has launched several CAR-T products commercially, yet none has made it onto the national reimbursement list; access runs instead through private insurance riders, instalment financing and manufacturer subsidies. The cure exists. The pathway to pay for it, for almost everyone, does not.
The fixes, part one: make it here
If the price is the problem, the most direct answer is to attack the price — and the boldest experiments in doing so are happening in Asia itself.
The emblem is NexCAR19. Developed by ImmunoACT, a company incubated at IIT Bombay in collaboration with Tata Memorial Centre, it became India's — and one of the world's first lower-middle-income country's — homegrown CAR-T therapies when it was approved in late 2023. Its launch price of roughly ₹30–42 lakh (about $36,000–50,000) is close to one-tenth of Western CAR-T list prices. And it is not a loss-leader: ImmunoACT reported profitability in its first full year, having treated more than 350 patients across some 70 hospitals, with the price drifting down toward ₹30 lakh as volume grew.
How did they do it? The company's leadership has been explicit that the decisive move was owning the intellectual property end to end rather than in-licensing constructs and vectors from higher-currency markets, which would have loaded licensing fees into the price. ImmunoACT manufactures its own lentiviral vector in-house — the gene-delivery component that can cost hundreds of thousands of dollars to buy in for even a small Western trial — and developed a cell-manufacturing process that avoids the most expensive automated equipment. It also "humanised" the CAR construct, which reduced the severity of cytokine release syndrome and neurotoxicity; fewer and milder complications mean lower downstream hospital costs, so the engineering choice was also a cost choice.
Korea offers the other localisation template. In early 2026, Curocell won approval for Rimqarto (anbalcabtagene autoleucel), the country's first domestically developed CAR-T therapy, for relapsed or refractory large B-cell lymphoma. The strategic prize there is partly logistical. Korean patients had previously needed their cells shipped abroad for manufacturing — a round trip that could take up to two months for someone with aggressive, fast-moving cancer. Curocell's GMP facility in Daejeon, paired with the first lentiviral-vector manufacturing site to win Korean GMP certification, is designed to cut the vein-to-vein time to roughly two weeks. The company is now negotiating national insurance coverage. Localisation here is not only about a lower sticker price; it is about turning a therapy that was geographically out of reach into one that can be delivered, quickly, at home.
Localisation, then, can genuinely collapse cost — but it matters which therapy. Autologous cell therapies like CAR-T are unusually amenable to it, because so much of the Western price is vector procurement, licensing and manufacturing overhead that local players can re-engineer. Complex in-vivo gene therapies — the AAV-delivered products like Zolgensma — are harder to cheapen this way, because the cost sits in vector production and the development burden of an ultra-rare indication. India's CMC Vellore haemophilia programme is the encouraging counter-example, demonstrating that an academic-public model can carry even a gene therapy through to durable results without a Western price tag attached. But the general lesson is sobering: "make it here" bends the curve dramatically for some modalities and only modestly for others.
The fixes, part two: change how you pay, not just what you pay
Price is one lever; payment structure is the other. If a system cannot absorb a multi-million-dollar cost in a single year, the obvious move is to spread it out — and to make sure it is only paying for cures that actually cure.
Two mechanisms have moved from theory to practice. Instalment models amortise the cost over several years, smoothing the budget shock; in the U.S., Zolgensma was offered to public payers as a five-year, five-instalment arrangement. Outcome-based agreements tie payment to whether the therapy works: the payer pays in full only if the patient hits predefined clinical milestones, and claws money back, or never pays it, if they do not.
Asia is quietly running some of the most instructive versions of these pilots. Taiwan's National Health Insurance Administration struck an outcome-based agreement with Novartis for Zolgensma in 2023 under which an expert panel reviews each case, efficacy is assessed against defined motor milestones over years, and the payer disburses in instalments tied to that performance — pushing the long-tail risk of failure back onto the manufacturer. In China, where no CGT has yet reached the national reimbursement list, the private market has improvised aggressively: collateral-backed interest-free instalment plans stretched over two years, one-time patient-assistance subsidies, and outcome-linked insurance products that refund six-figure sums (in renminbi) if a patient fails to achieve complete response within a set window. Japan, meanwhile, reimburses Zolgensma through its national scheme at a price set by benchmarking against the existing chronic therapy it displaces.
These models do real work. They convert an impossible lump sum into a tolerable annuity, and they protect a budget-constrained payer from buying a "cure" that relapses. South Korea's reimbursement system, which references European pricing and increasingly leans on managed-entry agreements, is structurally positioned to adopt them as its domestic CGT pipeline matures.
But the limits deserve honesty. Outcome-based contracts demand exactly what most Asian systems lack: durable, linkable patient registries to track outcomes over a decade, the administrative capacity to adjudicate each case, and continuity of coverage so a patient who switches insurers does not strand the contract. Instalments help with timing but not with the underlying total: a $2 million therapy paid over five years is still $2 million, which is why, on its own, novel financing nudges access at the margin rather than transforming it. The deeper fix pairs clever payment with a genuinely lower price — and with a third element that is easy to overlook: pooled, blended funds.
The fixes, part three: pool the money
The most promising structural idea is to stop asking any single payer to carry the cost alone. Dedicated CGT funds — capitalised by some mix of government, manufacturers, philanthropy and development finance — can ring-fence money for curative therapies, negotiate as a single large buyer, and spread risk across a larger pool than a hospital or even a province ever could.
Variants of this already exist in fragments across the region: government schemes that part-fund transplants and high-cost therapies, charitable and NGO networks that have for decades subsidised thalassaemia care and low-cost bone-marrow transplants (which Indian centres have delivered for a median of around $11,500, a fraction of the Western figure), and manufacturer patient-assistance programmes. The opportunity is to formalise and scale these into standing CGT access funds with predictable rules, rather than leaving patients to assemble financing case by case. Combined with local manufacturing to lower the unit price and outcome-based contracts to manage risk, a pooled fund is the closest thing to a complete answer the region has.
The equity question: cures for the few, or care for the many?
And yet the most uncomfortable question is not how to pay for these therapies, but whether — at the margin, with finite money — a system should.
The opportunity cost is stark in a way that is impossible to wave away. In a country spending roughly $74 per person per year on health, the sum required for a single imported gene therapy at Western list price could instead fund basic care for thousands of people, or a national thalassaemia screening and prevention programme that prevents far more disease than any number of individual cures can treat. Public-health economists make this point bluntly: a cure that reaches a few hundred patients can consume resources that might have extended or improved many thousands of lives spent elsewhere. The same edit that switches off one child's thalassaemia could, as carrier-screening and prenatal-counselling money, reduce the number of affected children born in the first place — a less photogenic intervention that may save more suffering per dollar.
This is not an argument against the therapies. It is an argument for seeing them clearly. The danger is a two-tier reality in which the science is celebrated as a national achievement while access is rationed to the urban, the insured and the connected — the patient who qualifies clinically but not financially, who is told a cure for their disease exists and is being manufactured in their own country, and who still cannot reach it. A therapy that exists but is unreachable can deepen inequity even as it advances medicine, by concentrating a society's scarce health resources and attention on the few who can be cured rather than the many who could be helped.
The honest resolution is that both things must happen at once. Prevention and basic care are not a substitute for cures, and cures are not a substitute for them. The systems that handle this well will be the ones that fund curative CGT and protect the unglamorous budgets — screening, transfusion safety, chronic-disease management — that serve the population at large, rather than letting the miracle cannibalise the baseline.
Can "make it here" actually bend the curve?
So: can localisation deliver on its promise?
The clearest verdict is that it already has, for the right modality. NexCAR19 is not a forecast; it is a commercial, profitable, indigenously manufactured CAR-T therapy treating hundreds of patients at roughly a tenth of the Western price, and Korea's Rimqarto shows the model is reproducible in a high-income Asian market with the added prize of slashing delivery times. For autologous cell therapies — where Western prices are inflated by licensing, imported vectors and manufacturing overhead that local innovators can genuinely re-engineer — "make it here" bends the curve steeply and demonstrably.
For complex in-vivo gene therapies, the curve bends less. The cost there lives in vector manufacturing and the brutal economics of ultra-rare diseases, and no amount of local assembly fully escapes it; CMC Vellore's haemophilia work suggests an academic-public route is possible, but it remains the exception, not yet the rule. And localisation does nothing, by itself, about the systems problem: even a $40,000 CAR-T is out of reach for a family living on a few thousand dollars a year, which is why local manufacturing only works as one leg of a tripod alongside novel financing and pooled funds.
The most realistic answer, then, is a qualified yes. Local manufacturing is necessary but not sufficient. It can take a therapy from "impossible everywhere" to "affordable for a health system and a middle class," which is a transformation worth celebrating — and it can do so while building exactly the domestic biotech capacity, supply chains and regulatory muscle that Asia will need for the next generation of these medicines. What it cannot do alone is reach the patient at the bottom of the income distribution, the one most likely to carry these diseases. Closing that final gap requires the price drop and the financing and the pooled fund and the political choice to protect baseline care while doing all of it.
The slide at the conference is real: these are cures, and they work. The spreadsheet down the hall is real too. Asia's distinctive contribution is to refuse to treat them as separate rooms — to insist that a therapy is not finished when it is proven, but when someone who needs it can actually get it. Whether the region can hold that line will determine whether the curtain-call applause was for a breakthrough that reached people, or for one that merely existed.
**Disclaimer:** This is an editorial draft built on publicly available data current as of mid-2026; therapy prices, approval statuses and health-spending figures are indicative and should be independently re-verified against primary sources before publication.
> Nothing here constitutes medical, financial, legal or investment advice — readers facing treatment or coverage decisions should consult qualified professionals.
Most Read
- Can APAC Biomanufacturing Decarbonise Without Pricing Itself Out?
- The Algorithm on the GMP Floor: AI Promises a Smarter Plant. Regulators Demand the Audit Trail.
- APAC's Peptide-Capacity Gamble
- After the Rush: APAC's mRNA and Vaccine Capacity Hangover
- The Biosimilar Race: Factory to the World — or Stuck in the Copycat Economy?
- The Vein-to-Vein Problem: Can APAC's Cold Chain Carry Advanced Therapies?
- Vectors, Plasmids and the CGT Trap: APAC's Cell and Gene Therapy Ambitions Face an Upstream Bottleneck
- Can APAC Build Radioligand Therapy Before the Atoms Decay?
- The Great Biopharma Reset: 50 Developments That Changed Everything in H1 2026
- Beyond the Trial: Can Real-World Evidence Earn Regulatory Trust in APAC?
- Beyond the Obvious Giant: Where APAC's Clinical Trials Go Next
- The Frontier That Won’t Quite Arrive
Bio Jobs
- Sanofi Turns The Page As Belén Garijo Steps In And Paul Hudson Steps Out
- Global Survey Reveals Nearly 40% of Employees Facing Fertility Challenges Consider Leaving Their Jobs
- BioMed X and AbbVie Begin Global Search for Bold Neuroscience Talent To Decode the Biology of Anhedonia
- Thermo Fisher Expands Bengaluru R&D Centre to Advance Antibody Innovation and Strengthen India’s Life Sciences Ecosystem
- Accord Plasma (Intas Group) Acquires Prothya Biosolutions to Expand Global Plasma Capabilities
- ACG Announces $200 Million Investment to Establish First U.S. Capsule Manufacturing Facility in Atlanta
- AstraZeneca Invests $4.5 Billion to Build Advanced Manufacturing Facility in Virginia, Expanding U.S. Medicine Production
News



